Does all activity reduce mortality or just exercise?
Backlinks: Training | WELL Rider Rewards Design
We start by defining exercise as intentional physical activity - analogous to logging as a “workout” on a wearable, versus passive exercise from, say, cooking.
In short, any activity level above sedentary is protective from all cause mortality, no need for it to be of moderate intensity. However, the benefits from light intensity are limited.
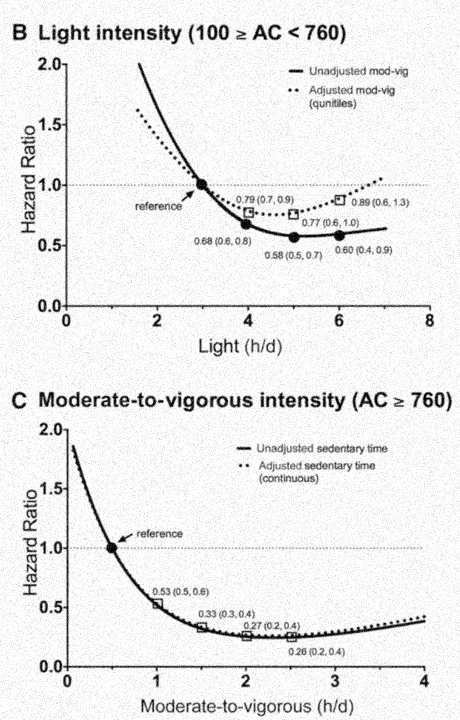 Fig. 1.
Benefits from light activity are real and substantial,
while moderate activity has further benefits [6].
Fig. 1.
Benefits from light activity are real and substantial,
while moderate activity has further benefits [6].
Figure 1 demonstrably supports that light intensity physical activity is hugely beneficial, while more intense physical activity provides further benefits: the light intensity HR hits .58 (a 40% reduction in mortality) as 5h/day, while the MVPA hits that RR with ~45min/day, exceeding it with .53 at 1hr/day and bottoming out at .26 RR (a nearly 75% reduction in deaths) with 2.5hrs/day of MVPA. In six words:
Some is good, more is better.
All in all, this supports us including all calories. A few notes:
- The exact # of MET-h to earn the full 1000 points is TBD. 15-h is probably too low since we're including light activity. I'll have to keep looking into this. See heading MET-h Target with Light Activity Included below.
- We are not dropping the connection to mortality by doing this, see the above mortality charts in Figure 1.
- In comparison with steps, including light activity calories is akin to including all steps with a step-based reward (we may not even know the intensity with which steps are taken). The reasons that calories are better than steps in general is because calories already do capture intensity and they work for exercises that don't have steps (biking, yoga, rowing). 100 steps is 100 steps. 100 steps running is more calories than 100 steps walking. So we are capturing intensity in this way, and rewarding is appropriately (more intense, more rewards).
- We're also not tying ourselves too closely to mortality here. This is striking a balance between mortality exactness and simplicity.
Potential ideas for capping/removing light activity
If we are talking about doing any "thresholding" at all (removing or capping the points of light activity), I think the best approach would be to limit the rewards possible from having only light intensity. The WELL points benefits could cap out where the mortality benefits cap out (while MVPA has more benefits beyond that). So it would be "1000 points total with up to 500 coming from light intensity". That said, I think we should just include all calories. This being a pilot, I think this is a minor detail (to cap light intensity rewards), that isn't worth solving for now.
While including light activity, we can monitor the data: if we see in the data that, say, 25% of people are earning all their rewards from only light intensity… then maybe we decide to use that learning to inform a future wearables program to include a cap on light intensity. But again, it's not essential for the pilot to work.
MET-h Target with Light Activity Included
The exact # of MET-h to earn the full 1000 points is TBD. 15-h is probably too low since we're including light activity. I'll have to keep looking into this.
This is an open task, still. It might be 22.5 MET-h, or 30 MET-h with all activity in the mix.
Idea: We can actually run through the whole NHANES dataset (3k people) to see where they land AND we can simulate a MM population from within NHANES by doing mock underwriting.
Dissenting research
However, some researchers claim that there is limited research on light intensity activity, with the (vast) evidence showing that at least moderate activity is associated with reductions in all cause mortality. From [1], we have
The precise type, amount, and intensity of physical activity required for protection needs further investigation. Traditional exercise recommendations suggest a threshold of activity that is necessary for protection, although current evidence does not support a dichotomous view of this issue. Clinical and epidemiological studies show a continuous dose-response gradient of outcome variables across a wide range of activity or fitness levels. Moderate amounts and intensities of physical activity are associated with improved health and reduced risk of morbidity and mortality when compared with low activity or fitness. The major public health emphasis for physical activity recommendations and programming should be to encourage the most sedentary and unfit 20 to 25% of the population to become at least moderately active, and this can yield substantial benefits for the population.
Still, in Powell (2011), they speculate:
Our guess is that light and moderate-intensity activities are important at the lower end (left) of the dose-response curve, where benefits are gained or lost more quickly; vigorous activities become important at the high end (right) of the curve, where changes in relative risk are slower.
In [2], they also do not see a lower bound on the physiological effects
Thus, for most individuals, the positive effects of regular exercise are exerted on blood lipids at low training volumes and accrue so that noticeable differences frequently occur with weekly energy expenditures of 1200 to 2200 kcal/wk. It appears that weekly exercise caloric expenditures that meet or exceed the higher end of this range are more likely to produce the desired lipid changes.
References
- Blair SN, Connelly JC. How much physical activity should we do? The case for moderate amounts and intensities of physical activity. Res Q Exerc Sport. 1996 Jun;67(2):193-205. doi: 10.1080/02701367.1996.10607943. PMID: 8835998.
- Durstine JL, Grandjean PW, Davis PG, Ferguson MA, Alderson NL, DuBose KD. Blood lipid and lipoprotein adaptations to exercise: a quantitative analysis. Sports Med. 2001;31(15):1033-62. doi: 10.2165/00007256-200131150-00002. PMID: 11735685.
- Durstine JL, Grandjean PW, Cox CA, Thompson PD. Lipids, lipoproteins, and exercise. J Cardiopulm Rehabil. 2002 Nov-Dec;22(6):385-98. doi: 10.1097/00008483-200211000-00002. PMID: 12464825.
- Keller C, Treviño RP. Effects of two frequencies of walking on cardiovascular risk factor reduction in Mexican American women. Res Nurs Health. 2001 Oct;24(5):390-401. doi: 10.1002/nur.1039. PMID: 11746068.
- Lee IM, Skerrett PJ. Physical activity and all-cause mortality: what is the dose-response relation? Med Sci Sports Exerc. 2001 Jun;33(6 Suppl):S459-71; discussion S493-4. doi: 10.1097/00005768-200106001-00016. PMID: 11427772.
- Matthews, et. al. Accelerometer-measured dose-response for physical activity, sedentary time, and mortality in US adults, 2016.